MKSAP Quiz: History of diffuse headache, fatigue
A 27-year-old woman is evaluated in the emergency department for a 2-day history of diffuse headache, fatigue, and gingival bleeding on brushing her teeth. She is otherwise healthy. Her only medication is an oral contraceptive, and medical and family histories are unremarkable.
On physical examination, she is alert and oriented but reports having a headache. Funduscopic examination is normal. There are a few scleral hemorrhages, and mild icterus is noted. Petechiae that had gone unnoticed by the patient are visible on the lower extremities. Cardiopulmonary and abdominal examinations are normal.
Laboratory studies:
| Hemoglobin: | 8 g/dL (80 g/L) |
| Platelet count: | 34,000/µL (34 × 109/L) |
| Reticulocyte count: | 12% of erythrocytes |
| INR: | 1.1 |
| Activated partial thromboplastin time (aPTT): | 32 s |
| Thrombin time: | 16 s (control, 15 s) |
| Lactate dehydrogenase: | 2000 U/L |
| Serum creatinine: | 0.8 mg/dL (61 µmol/L) |
| D-dimer assay: | Negative |
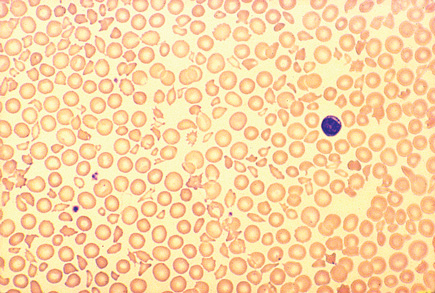
A peripheral blood smear is shown.
Which of the following is the most appropriate next step in management?
A. aPTT mixing study
B. Direct antiglubulin (Coombs) test
C. Intravenous immune globulin
D. Plasma exchange
E. Platelet antibody test
Answer and critique
The correct answer is D: Plasma exchange. This question can be found in MKSAP 15 in the Hematology and Oncology section, item 23.
This patient has evidence of microangiopathic hemolytic anemia, thrombocytopenia with normal coagulation, and central nervous system symptoms, the principal triad of thrombotic thrombocytopenic purpura (TTP); renal failure and fever compose the pentad of symptoms. Plasma exchange is the principal treatment modality for TTP and should be initiated as soon as possible to decrease patient morbidity. Plasma exchange reverses the platelet consumption that is responsible for the thrombus formation causing the findings associated with TTP. It is acceptable to initiate plasma exchange even in circumstances when the diagnosis is in question, only to be stopped when an alternative diagnosis is established.
Intravenous immune globulin is useful in treating patients with immune thrombocytopenic purpura (ITP) but not TTP. The presence of severe microangiopathic hemolytic anemia is inconsistent with ITP and, therefore, precludes the use of intravenous immune globulin in this patient.
A direct antiglobulin (Coombs) test would be appropriate for patients with suspected immune hemolytic anemia, but this is a case of microangiopathic hemolytic anemia as evidenced by schistocytes on the peripheral blood smear.
An activated partial thromboplastin time (aPTT) mixing study is not indicated in this patient because her aPTT is normal.
Platelet antibody assays are generally not very sensitive or specific in patients with thrombocytopenia and would not be helpful in this case. A positive test result would not explain the presence of schistocytes on the peripheral blood smear.
Key Point
- Microangiopathic hemolytic anemia, thrombocytopenia with normal coagulation, and central nervous system symptoms are the principal triad of thrombotic thrombocytopenic purpura; renal failure and fever compose the pentad of symptoms.


