MKSAP Quiz: Diabetic ketoacidosis
A 27-year-old black man is admitted to the hospital following his first episode of diabetic ketoacidosis. The patient has also had bacterial sinusitis for which he has been taking trimethoprim-sulfamethoxazole for the past 4 days. He has also noticed that his urine is dark. Additional medications are lispro and glargine insulins.
On physical examination, the patient appears to be uncomfortable. He has scleral icterus. Temperature is 37.8°C (100.2°F), blood pressure is 127/66 mm Hg, pulse rate is 112/min, and respiration rate is 25/min. Tachycardia is heard on cardiac auscultation, but cardiac examination is otherwise unremarkable. Abdominal examination discloses diffuse abdominal tenderness but no hepatosplenomegaly.
Laboratory studies:
| Hemoglobin: | 10.2 g/dL (102 g/L) |
| Reticulocyte count: | 11% of erythrocytes |
| Lactate dehydrogenase: | 1145 U/L |
| Total bilirubin: | 5.1 mg/dL (87.2 µmol/L) |
| Indirect bilirubin: | 4.6 mg/dL (78.7 µmol/L) |
| Urinalysis: | 3+ ketones, 3+ bilirubin |
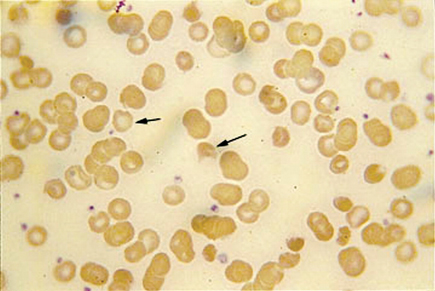
A peripheral blood smear is shown.
Which of the following is the most likely diagnosis?
A. Glucose 6-phosphate dehydrogenase (G6PD) deficiency
B. Hereditary spherocytosis
C. Microangiopathic hemolytic anemia
D. Warm antibody-mediated hemolytic anemia
Answer and Critique
The correct answer is A: Glucose 6-phosphate dehydrogenase (G6PD) deficiency. This question can be found in MKSAP 15 in the Hematology and Oncology section, item 3.
Glucose 6-phosphate dehydrogenase (G6PD) deficiency is the most common disorder of erythrocyte metabolism. G6PD is necessary for generating adequate nicotinamide adenine dinucleotide phosphate-oxidase (NADPH) to prevent oxidant stress. G6PD is found on the X-chromosome, and deficiency, therefore, occurs rarely in women.
Several G6PD variants are detected electrophoretically, including G6PD B, the wild-type enzyme; and G6PD A−, which is responsible for oxidative hemolysis in aged erythrocyte cells. The acute onset of symptoms and findings in patients with this deficiency can be precipitated by drugs, infection or diabetic ketoacidosis. In this patient, hemolysis was likely precipitated by diabetic ketoacidosis and trimethoprim-sulfamethoxazole.
At 2 to 4 days after introduction of the oxidative stress in patients with G6PD deficiency, there is the onset of jaundice and dark urine, with or without abdominal and back pain. The hemoglobin concentration decreases by 3 to 4 g/dL (30 to 40 g/L), and there is an appropriate increase in reticulocytes. The hemolysis spontaneously resolves in approximately 1 week as the older enzyme-depleted cells are replaced by new cells with sufficient G6PD to prevent further hemolysis. Additional laboratory findings in patients with G6PD deficiency include a negative direct and indirect anti-globulin (Coombs) test and the presence of “bite” or “blister” cells produced when accumulated oxidized hemoglobin remains adherent to the erythrocyte membrane with an adjacent membrane-bound clear zone. Such cells are visible on this patient's peripheral blood smear. Because reticulocytes can have normal G6PD levels in patients with the G6PD A− phenotype, measuring G6PD levels during an acute episode may produce a false-negative result.
Patients with warm antibody-mediated hemolysis have spherocytes on the peripheral blood smear as do patients with hereditary spherocytosis. The direct antiglobulin test is positive in patients with warm antibody-mediated hemolysis and negative in patients with hereditary spherocytosis. Patients with a microangiopathy have schistocytes on the peripheral blood smear and, typically, a low platelet count. Neither of these findings is present in the peripheral blood smear shown.
Key Point
- Because reticulocytes can have normal G6PD levels in patients with the G6PD A− phenotype, measuring G6PD levels during an acute episode may produce a false-negative result.